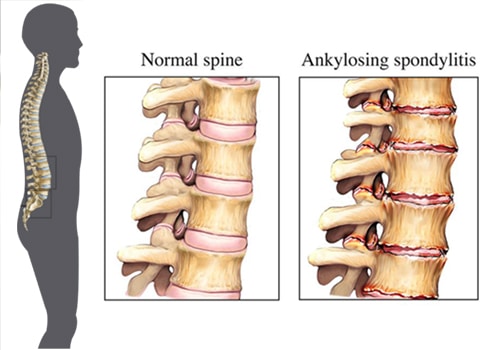
ANKYLOSING SPONDYLITIS
DIGNOSTIC CRITERIA
Definition: A chronic progressive inflammatory disease of spinal joints sacroiliac, hip, shoulder, occasionally peripheral joints.
- Clinical features include low back pain and stiffness especially in the mornings which gets better with activity, as opposed to mechanical back pain due to disc problems which lessen with rest but increase with activity. Lumbar spine motions diminished universally. Progressive with other joint involvement and ultimately in 10 years the patient develops thoracic lumbar kyphosis and restrictive chest wall movements.
- Raised ESR, Absent RA, and HLA-B27 tissue antigen present.
- Complications include Aortic root dilatation, Aortic incompetence, and Anterior uveitis.
- Sclerosis of SI joints, calcification of spinal ligaments, and squaring of osteoporotic spine (‘Bamboo spine”) occurs in many patients ad cannot be predicted or prevented.
- Osteoporosis can develop in the fused spondylitic spine giving rise to pathologic fractures.
Some patients might have cauda equina syndrome with bowel and bladder involvement.
Prognosis : Varies with almost all patients having persistent symptoms throughout, but about 10% jet very disabled in 10 years. Prognosis good if mobility and upright posture are maintained. Early (<2 years) hip involvement portends poorer prognosis. The impact of therapy on disease progression is unknown as disease may evolve slowly over 20 years.
MANAGEMENT
General Principles
- Treatment focuses on control of inflammation to maintain spinal mobility. NSA IDS seem an effective sheet anchor in pain control. Plus an exercise programme designed to maintain posture and mobility, which is the key to management.
- Sacroiliac involvement is the hallmark, and 20-30% have peripheral joints involved as well. Mostly in young men in 2’ and 3 decades, and strong association with HLA-B 27 antigen.