BRONCHIAL ASTHMA
DIAGNOSTIC CRITERIA
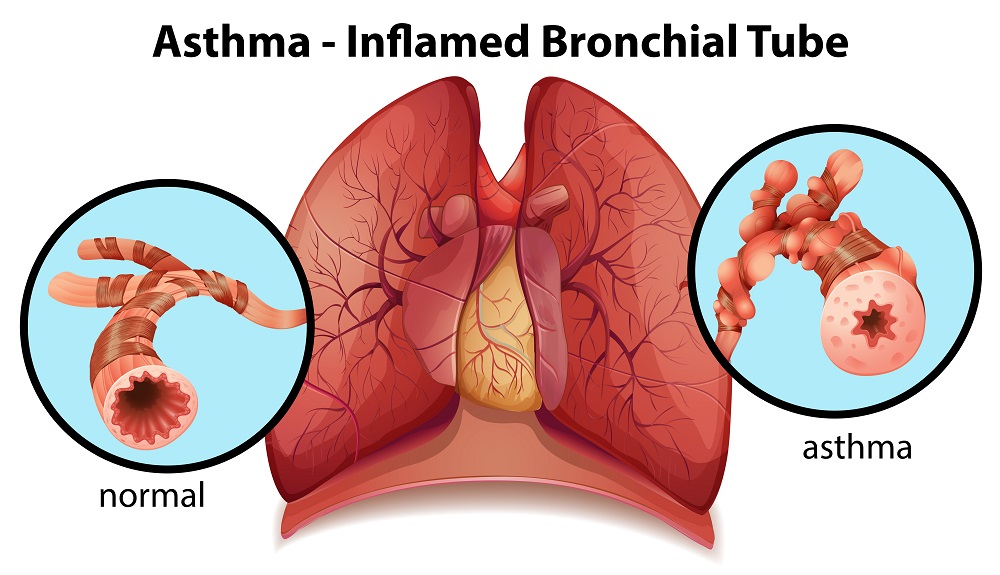
Definition: Is a chronic, intermittent, inflammatory disease of the airways characterised by episodes of wheezing, coughing, breathlessness and chest-tightness. It is usually reversible but can be severe and occasionally fatal.
- It is a very common respiratory problem afflicting about 5— 10% % of populations and affecting all age groups. Increasing prevalence worldwide.
- Episodic or chronic wheezing, dyspnoea, cough, and tightness in the chest.
- Spasm of bronchial smooth muscle leading to narrowing of large and small airways, with oedema, and inflammation of the bronchial mucosa with production of mucous.
- Tending to occur in families, this bronchial hyper-responsiveness is triggered by a variety of causes including cold air, smoke, exercise, emotion, infection, pollen, house dust (mites), gastrooesophageal reflux, sleep, etc.
- Complete or partial, reversibility of the obstructive dysfunction with bromcho-dilator therapy.
- Pulmonary function tests are essential for diagnosis of bronchial asthma. PETs show an obstructive pattern with a decrease in expiratory flow rates. There is a decrease in the FEVI/FVC ratio. Supportive of the diagnosis, the obstructive pattern improves after bronchodilator therapy.
- Prognosis: Good in 95% of chronic asthmatics. There has been some increase in asthma morbidity ad mortality in recent times. Younger patients with extrinsic asthma do best. Rigorous medical regimens can reduce hospital admissions.
- Prognosis in acute episode is poor in the presence of (a) active accessory muscles, (b) poor response to initial treatment, (c) disturbance of consciousness, (d) disappearance of wheezing in a profoundly fatigued patient, (e) low Pao2, (f) rising Pco2, and (g) presence of complications like pneumothorax, atelectasis.
MANAGEMENT
General principles:
- The current approach to treatment of asthma emphasises ‘Prevention’ with the goal being the decrease o the bronchial hyperresponsiveness, avoidance of allergens where ver possible, and chronic use of anti-inflammatoty drugs including corticosteroids and Cromolyn sodium. Inhalational steroids are the cornerstones in the management of persistent moderate and severe asthma today. Also, they are used prophylactically in patients who use beta stimulant more than once daily.
- The patient’s seff-monitoring and self-treatment is important factors in reducing morbidity and mortality. Acute episodes, as in the earlier times, get treated with brorichodilators, corticosteroids, antichollnergics and oxygen as needed. Treatment of bronchial asthma is mostly as outpatient, unless bronchospasm is unrelieved by xanthines, B agonists and steroids.
- Leukotriene inhibitors introduced recently are not to be used for relieving acute episodes of asthma, but often help reduce the dose of inhalational steroids, but not necessarily.
- Metered dose inhalers (MDI) need coaching in proper technique in use - To breathe out first, then activate the inhaler at the beginning of inhalation, (the inhalation should take about 5 seconds), and then breath-holding for at least 10 seconds, before letting out the air. Mouth rinsing is recommended after each inhalation. A large number of asthma sufferers do not use the aerosols properly.
- Measurement of PEFR helps assess severity of episode as well as the response to therapy. Home monitoring can be easily taught to the patient.
- Today, for those with poorly controlled asthma on inhaled steroids, addition of a long acting B2-agonist like salmeterol is the best option available. For those with repeated acute exacerbations, it would be best to increase the dose of inhaled steroids, or a combination of both strategies. Long acting B2-agonist as monotherapy is not recommended.
Peak flow meters, Spacer and Nebulisers
- Peak flow meters that measure peak flow are of great use for patients with moderate to severe asthma as it guides them in measuring fall in their peak-flow. Guides them in management regards dose of drugs, frequency of administration and need for hospitalization when indicated. They would need initial coaching from their physicians on use and interpretation. (See peak flow values under tabulation).
- Spacer devices for use with inhalational drugs are of most use for patients with poor inhalation technique, requiring high doses of inhalational drugs, for children, those that develop oral candidiasisi with inhalational steroids, and patients with nocturnal asthma. Devices that are large in size are the most useful. The patient should inhale as quickly as possible after the actuation.
- Nebulisers convert the solution of a drug into aerosol. In asthma beta adrenergic stimulants Ipratropium, Cromoglycate and steroids are used through nebulisers. The patient should be aware that the dose of broncho-dilator given through a nebuliser is much higher than from an aerosol inhaler. The indications for nebuliser inhalational therapy are:
- Those with chronic daily wheeze responsive to such therapy without side effects.
- In acute exacerbation or airway obstruction.
- As regular therapy for severe asthmatic needing higher dose therapy.
- For children needing inhalational steroid or cromoglycate.
- Patient education in proper use of the nebuliser is very essential if, as usually the patient uses it at home.
General Measures
-
-
- Home monitoring of PFR- To report to doctor if PFR drops below 70% of baseline.
- Eliminating irritants.
- Hyposensitisation.
- Ensuring adequate hydration.
- Attention to general health measures.
Patient teaching
-
-
-
- Proper use of MDI.
- Home monitoring of PFR and to report if it falls below 70%
- Avoid iced drinks, spicy foods, and cold immersion.
- Keep living and bed room as dust free as possible
- Avoid exercise in exercise Induced asthma.
- Avoiding allergens like dust, smoke, emotional upsets and special foods.
- Breathing exercises, especially yoga.
- Avoid aspirin, tartrazine and sulfites (preservatives).
- Drink plenty of fluids and avoid; dehydration.
Follow-up
Prearranged plan for any exacerbations. It should be remembered that after an exacerbation the bronchial hyper-reactivity persists for 4-6 weeks.