CHROMC OBSTRUCTIVE PULMONARY DISEASE (COPD)
COPD, a term usually referring to a combination of Chronic Bronchitis and Emphysema.
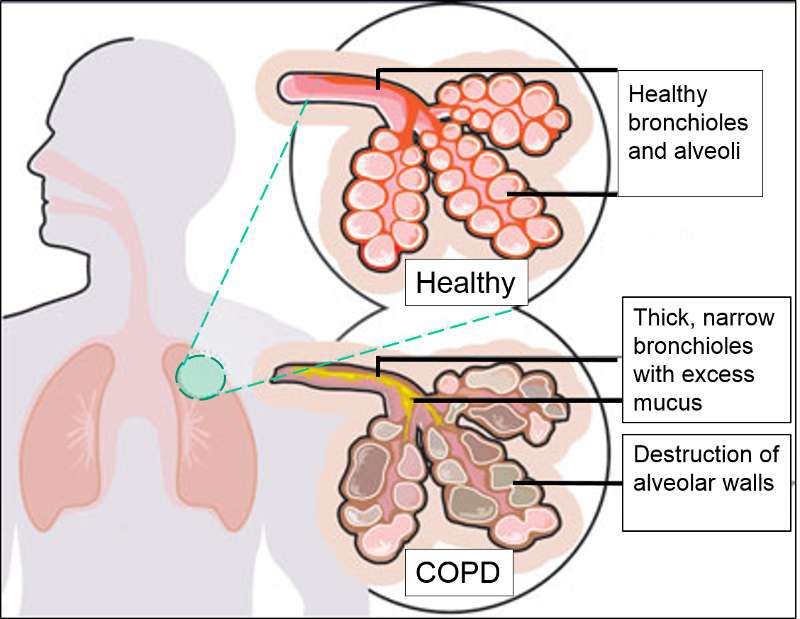
- Productive cough for 3 months or more for at least 2 years preceding, and not due to any other disease. (Chronic Bronchitis)
- Abnormal and permanent enlargement of air spaces beyond the terminal bronchiole with destruction of their walls and without obvious fibrosis (Emphysema).
- Cigarette smoking is the most important cause in most cases, though only <15% of smokers develop COPD. Other causes include air-pollution, polluted enclosed kitchens as in the cooler parts of India, occupational exposures, alpha I anti-tyrosirie deficiency etc.
- Clinical features of chronic bronchitis (Type B, the “blue bloater” ) are cough, wheezing, sputum production, recurrent infections and later, pedal oedema. There is always a bronchospastic element. Clinical features of emphysema are dyspnoea, barrel chest, diminished breath sounds, pursed lips and accessory muscles use in breathing (Type A, the” pink puffer” ). They occur together to variable degree.
- Lung function tests reveal low FVC, decreased FEV1 value with concomitant reduction of FEV1! FVC ratio. In the emphysematous patient, despite the dyspnea, the gas exchange is essentially preserved with minimal hypoxaemia and normal PaCO2, but there is increased total lung and residual volumes. Chest film shows increased broncho-vascular markings in Chronic bronchitis, and small heart with hyper-infla ted lungs in Emphysema.
Prognosis : Worse with advancing age, poor post-broncho-dilator FEV1, in those that continue to and in those in poor nutrition. Following initial episode of respiratory failure 5 year survival is only 25%. Development of cor pulmonale, hypercapnia and persistent tachycardia are poor prognostic indic tors.